





Abstract
We investigated the effects of both ambient air pollution and traffic noise on adult asthma prevalence, using harmonised data from three European cohort studies established in 2006–2013 (HUNT3, Lifelines and UK Biobank).
Residential exposures to ambient air pollution (particulate matter with aerodynamic diameter ≤10 µm (PM10) and nitrogen dioxide (NO2)) were estimated by a pan-European Land Use Regression model for 2007. Traffic noise for 2009 was modelled at home addresses by adapting a standardised noise assessment framework (CNOSSOS-EU). A cross-sectional analysis of 646 731 participants aged ≥20 years was undertaken using DataSHIELD to pool data for individual-level analysis via a “compute to the data” approach. Multivariate logistic regression models were fitted to assess the effects of each exposure on lifetime and current asthma prevalence.
PM10 or NO2 higher by 10 µg·m−3 was associated with 12.8% (95% CI 9.5–16.3%) and 1.9% (95% CI 1.1–2.8%) higher lifetime asthma prevalence, respectively, independent of confounders. Effects were larger in those aged ≥50 years, ever-smokers and less educated. Noise exposure was not significantly associated with asthma prevalence.
This study suggests that long-term ambient PM10 exposure is associated with asthma prevalence in western European adults. Traffic noise is not associated with asthma prevalence, but its potential to impact on asthma exacerbations needs further investigation.
Abstract
Long-term ambient PM10 exposure is associated with asthma prevalence in three European adult cohorts http://ow.ly/En4b3049S7X
Introduction
Asthma is a complex respiratory illness which affects both children and adults. Globally, asthma was the 28th leading cause of disability-adjusted life-years in 2010 [1] and it was estimated in 2014 that around 334 million people worldwide had asthma [2]. An increasing prevalence of asthma was seen in some parts of the developed world at least until the late 1990s, after which the temporal trend varied across countries [3]; in some regions, the asthma epidemic continues to increase in adults [4].
Some potential risk factors have been identified for these prevalence trends. One is exposure to air pollution, which has a role in exacerbations of pre-existing asthma and affects asthma morbidity via various mechanistic pathways, including airway hyperresponsiveness, airway remodelling, oxidative stress and immune responses [5]. However, previous studies are inconsistent with respect to the associations between long-term air pollution and asthma prevalence [6] and incidence [7]. In adults, some studies reported positive associations between self-reported traffic intensity and asthma prevalence, although these findings were not supported by analysis of individual modelled exposures to air pollution in the same populations [8, 9]. Other studies did not report significant associations of air pollution and adult asthma prevalence [10–15], except for one [16]. A few studies investigated the effect of air pollution on adult-onset asthma, with significant associations reported either among all participants [17, 18], never-smokers [19] or females only [20]. An analysis of six European cohorts reported positive but nonsignificant associations of asthma incidence with a range of modelled air pollutants [21].
Another asthma risk factor is chronic psychosocial stress, which may affect asthma morbidity through biological responses and disease management [22]. To the best of our knowledge, there are no studies investigating whether individual exposure to traffic noise, generally seen as an environmental stressor and mostly coexisting with air pollution in road traffic settings, would affect adult asthma morbidity. Only two previous small studies investigated associations between subjective noise exposures and asthma prevalence, with null results reported [23, 24].
In this study, we investigated the separate and joint effects of both long-term air pollution and traffic noise exposure on adult asthma prevalence, using a pooled individual-level analysis of harmonised data from three recently established large European cohort studies: HUNT3 (Norway) [25], Lifelines (the Netherlands) [26] and UK Biobank (UK) [27].
Methods
Study populations
Three cohort studies participating in BioSHaRE (Biobank Standardisation and Harmonisation for Research Excellence in the European Union) were included in this study.
HUNT3 is the third survey of the HUNT (Helseundersøkelsen i Nord-Trøndelag) study, based in Nord-Trøndelag County in Norway [25]. During 2006–2008, data from 50 805 residents aged ≥20 years were collected by trained staff. Lifelines is a multidisciplinary prospective population-based cohort study examining in a three-generation design the health and health-related behaviours of 167 729 individuals living in the north of the Netherlands [26]. During baseline recruitment (2006–2013), residents aged 25–50 years and family members registered in general practices were randomly invited to participate. Quality-checked data on 93 277 Lifelines participants were available within the timeframe of this study. UK Biobank, established during 2006–2010, recruited 502 649 participants aged 40–69 years across the UK [27].
Exposure assessment
Ambient air pollution
A pan-European Land Use Regression (LUR) model at a resolution of 100×100 m was used to assign annual air pollution estimates at the home address for each participant from the three cohorts [28]. Annual mean nitrogen dioxide (NO2) and particulate matter with aerodynamic diameter ≤10 µm (PM10) concentration data during 2005–2007 were obtained from over 1500 monitoring sites across Europe; means for 2007 were used in the analyses as data for both pollutants were available for that year for all three cohorts. Only monitoring sites which captured over 75% of the total hours for NO2 and days for PM10 were included. The pan-European LUR model was developed using 80% of these monitored air pollution data, satellite-based ground-level concentrations of NO2 and particulate matter with aerodynamic diameter ≤2.5 µm (PM2.5) on a 10-km grid, and land use and traffic variables obtained from a geographical information system (online supplementary material S1). Model performance (explained variance (R2) between modelled and measured exposures) for PM10 and NO2 estimates was 36–48% and 46–56%, respectively, evaluated against the independent subset (20%) of all included monitoring sites [28].
Additional address-level annual estimated NO2 and PM10 concentrations for 2010 were available for Lifelines and UK Biobank, using LUR models for the respective study areas from the ESCAPE (European Study of Cohorts for Air Pollution Effects) project [29, 30]. R2 for PM10 and NO2 ESCAPE-LUR models was 60–88% and 81–87%, respectively, as evaluated using the leave-one-out cross-validation method [29, 30].
Traffic noise
We used a simplified version [31], with some lower resolution inputs, of the CNOSSOS-EU (common noise assessment methods in European Union) noise modelling framework [32] to estimate noise exposures at the address level for participants in each study. In brief, noise sound level was estimated for all roads within 500 m of the home address, with consideration of noise propagation due to refraction and diffraction, absorption from buildings, distance, and angle of view. Road network geography, hourly vehicle flows, building heights, land cover and meteorological data were obtained for the respective study areas. For participants living on minor roads that were not captured in the national-level traffic datasets, we assigned a fixed low-level baseline flow. Traffic data were for 2009 and land cover data were for 2006.
For all three cohorts, we modelled annual mean A-weighted sound pressure level in decibels (dB(A)) for day-time noise (averaged sound level from 07:00 to 19:00 h) and night-time noise (averaged sound level from 23:00 to 07:00 h).
Harmonisation of covariates and outcomes
Age, sex, body mass index (BMI), education level (primary school or less, secondary school, or post-secondary school or above), paid employment (yes or no), smoking (current smoker, ex-smoker or never-smoker) and years at baseline address were harmonised retrospectively across cohorts (online supplementary material S2) following a validated protocol [33].
Lifetime asthma prevalence (“ever-had asthma”) was harmonised based on the self-reported answers (yes or no) in the study questionnaire (table 1). “Current asthma” was defined as a self-report of ever-had asthma and participant reporting asthma-related medication use, for which data were ascertained differentially in each cohort (table 1).
Information on ever-had asthma and asthma-related medication by each cohort
We did not have information on incident asthma.
Statistical analyses
To overcome the ethico-legal issues associated with physical sharing of data, statistical analyses were performed using DataSHIELD [34], a novel tool which allowed co-analysis of harmonised datasets across the three participating cohorts without physically sharing the individual-level data.
First, we calculated Spearman correlations between metrics of air pollution and noise for each cohort. Associations between each metric of air pollution (or noise) and ever-had asthma and current asthma were analysed using multivariate logistic regression. Both air pollution and noise metrics were analysed on a continuous scale, assuming a linear effect. Additionally, three categories for day-time noise (<55, 55–60 and ≥60 dB(A)) and night-time noise (<45, 45–50 and ≥50 dB(A)) were used.
The covariates were chosen a priori based on current knowledge. The sequence of models was: adjusted for study (Model 1), adjusted for study, age and sex (Model 2), and further adjusted for BMI, smoking, education level and employment status (Model 3). Based on Model 3, road traffic noise (or air pollution) was additionally added to the air pollution (or noise) model.
Sensitivity analyses were conducted based on Model 3: 1) restricting analyses to those living at the same address for ≥10 years, 2) using ESCAPE-LUR air pollution metrics (PM10 and NO2) for Lifelines and UK Biobank instead of the pan-European LUR metrics, and 3) conducting study-specific analyses and then pooling estimates using meta-analysis methods, in both fixed-effect and random-effect models, to explore heterogeneity [35].
Stratified analyses were conducted based on Model 3 by: 1) sex, 2) age <50 or ≥50 years, 3) smoking status, 4) BMI <25, 25–30 or ≥30 kg·m−2 and 5) education level.
Individual-level fixed-effect pooled analyses were performed in DataSHIELD version 4.1.2 (www.datashield.ac.uk). Study-level meta-analyses were performed in Stata version 12.1 (www.stata.com).
Results
Overall, prevalence of ever-had asthma was 11.1% and prevalence of current asthma was 4.3% (table 2). Prevalence of ever-had asthma or current asthma was higher among females, those aged <50 years, with a BMI >25 kg·m−2 and less educated.
Prevalence of ever-had asthma and current asthma by each subgroup for each cohort and for the pooled dataset
Mean±sd PM10 ranged from 11±1.1 (HUNT3) to 24±1.7 (Lifelines) µg·m−3, while NO2 ranged from 13±3.9 (HUNT3) to 31±10.7 (UK Biobank) µg·m−3 (online supplementary material S3). Pooling data for PM10 and NO2 from 606 657 and 608 102 participants, respectively, median (interquartile range (IQR)) PM10 was 23 (4.3) µg·m3 and NO2 was 29 (11.4) µg·m3 (online supplementary material S3). In the pooled data, median (IQR) day-time noise and night-time noise estimates were 59 (4.3) and 49 (4.2) dB(A), respectively.
Spearman correlations between PM10 and day-time noise ranged from r=0.04 (HUNT3) to 0.38 (Lifelines), and between NO2 and day-time noise ranged from r= −0.05 (HUNT3) to 0.43 (Lifelines) (online supplementary material S4). Correlation between NO2 and PM10 was r=0.8, and between day-time and night-time noise r=0.99 in each of the three cohorts.
In all models, statistically significant associations were found for PM10 and NO2 in relation to prevalence of ever-had asthma (table 3). In the fully adjusted Model 3, PM10 higher by 10 µg·m−3 was associated with 12.8% (95% CI 9.5–16.3%) higher prevalence of ever-had asthma and 6.4% (95% CI 1.2–11.9%) higher prevalence of current asthma. NO2 higher by 10 µg·m−3 was associated with 1.9% (95% CI 1.1–2.8%) higher prevalence of ever-had asthma, but not current asthma prevalence. Further adjustments for day-time noise did not change the associations.
Associations between ambient air pollution (pan-European Land Use Regression modelled particulate matter with aerodynamic diameter ≤10 µm (PM10) and nitrogen dioxide (NO2)) and asthma prevalence: pooled individual-level analyses from three cohorts
No associations between categorical or continuous noise exposures and asthma prevalence were seen (table 4 and online supplementary material S5).
Associations between categorical day-time noise (07:00–19:00 h), night-time noise (23:00–07:00 h) and asthma prevalence in Model 3: pooled individual-level analyses from three cohorts
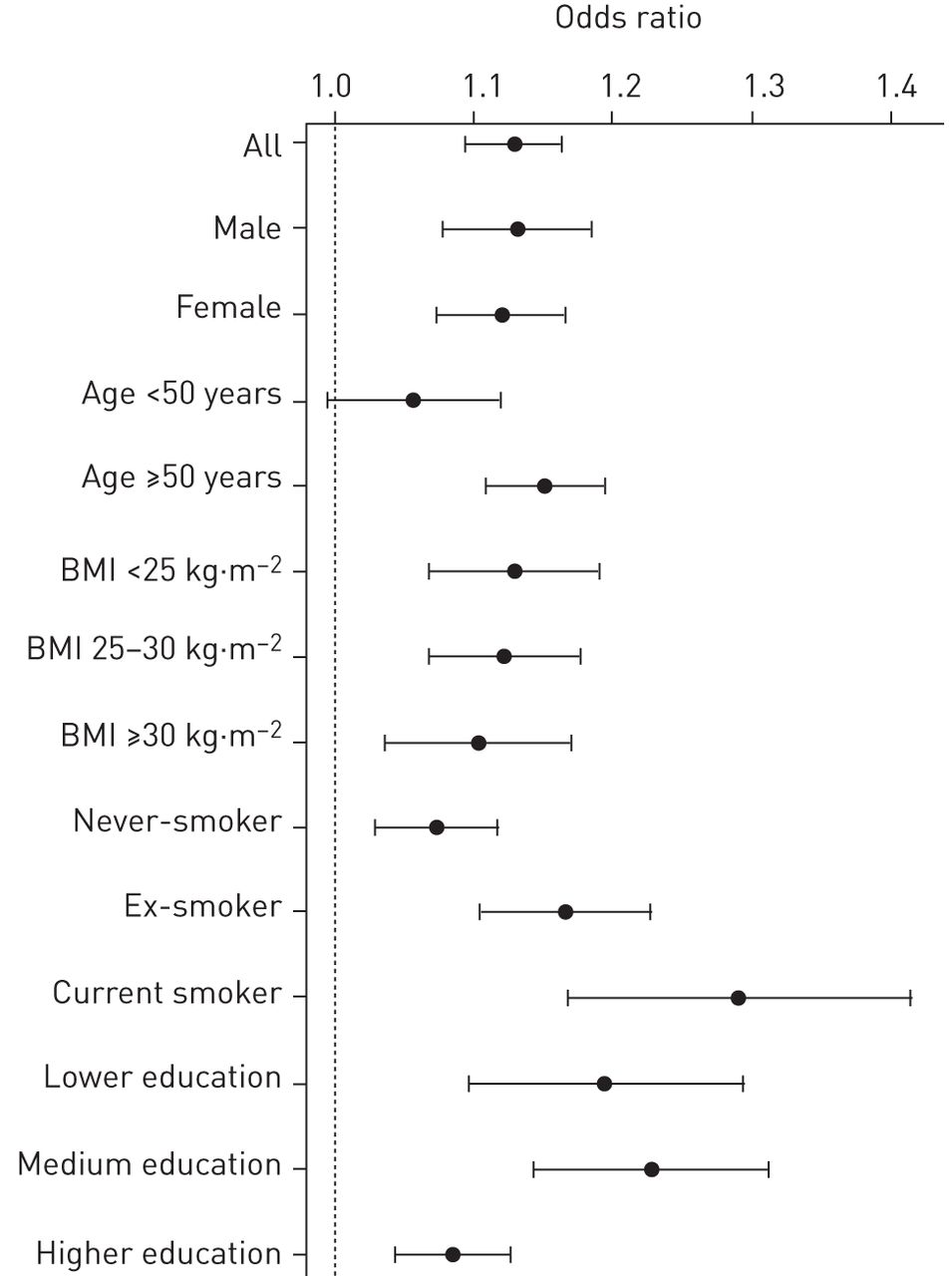
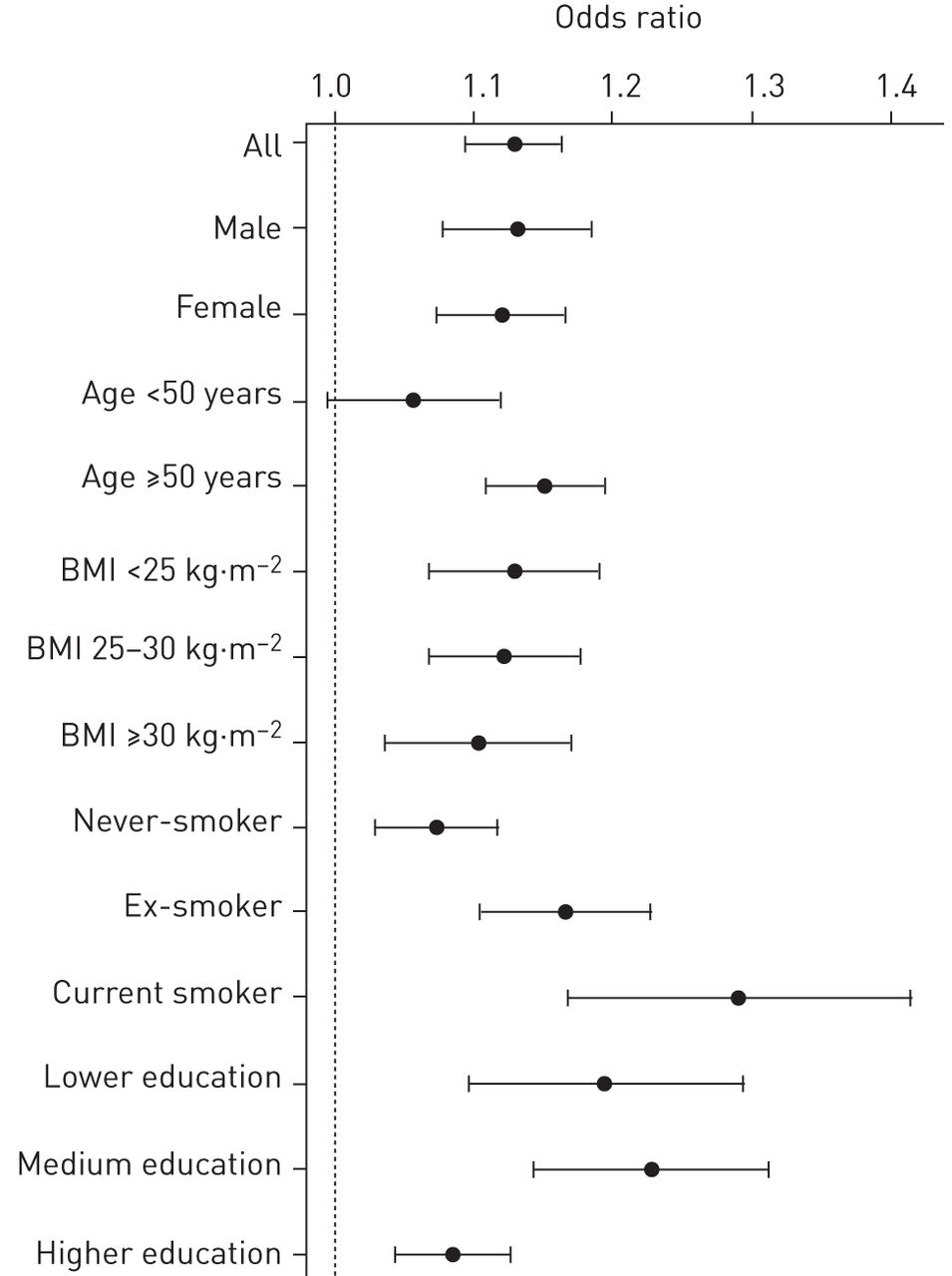
Significant effect modifications (p-value for interaction <0.01) by age, smoking and education were observed between PM10 and ever-had asthma prevalence, with stronger associations seen for those aged ≥50 years, ever-smokers and less educated (figure 1). Similar findings were observed for current asthma (online supplementary material S6). No significant effect modifications were seen between NO2 and ever-had or current asthma prevalence by any of the studied variables (online supplementary material S6).
{kind=link}
Associations between pan-European Land Use Regression modelled particulate matter with aerodynamic diameter ≤10 µm (PM10) (per 10 µg·m−3) and prevalence of ever-had asthma: subgroup analyses based on Model 3 (adjusted for study, age, sex, body mass index (BMI), smoking status, education level and employment status). Bars show 95% confidence intervals.
In sensitivity analyses, for participants living at the same address for ≥10 years, associations between PM10, NO2 and ever-had asthma became slightly stronger (online supplementary material S7). Using ESCAPE-LUR modelled PM10 and NO2 for Lifelines and UK Biobank instead of the pan-European LUR metrics, both ever-had asthma and current asthma prevalence were significantly associated with both PM10 and NO2 (online supplementary material S7).
Associations between NO2, PM10, day-time noise and ever-had asthma prevalence in Model 3 assessed via meta-analysis across cohorts (supplementary figure S1) were similar to those from the individual-level analysis. However, study-specific associations between NO2, PM10 and current asthma prevalence were heterogeneous (p<0.05) (supplementary figure S2), and none of the pooled study estimates in the meta-analyses were significant. The effect size in the meta-analyses was dominated by UK Biobank.
Discussion
In this cross-sectional study involving three large European cohorts, there was a statistically significant positive association between ambient PM10 air pollution and both ever-asthma and current asthma prevalence. NO2 was significantly associated with ever-asthma but not current asthma. We found no association between traffic noise exposures and ever-had or current asthma prevalence.
This study is one of the largest studies of its kind to date. Harmonised exposures and health data of over 600 000 participants from three cohorts were brought together for an integrative pooled individual-level analysis, using DataSHIELD. Both air pollution and noise exposures were modelled at the home address, providing an opportunity to investigate health effects of both exposures in the same study.
Previous findings
Only a few studies have investigated the role of air pollution on adult asthma prevalence, with most finding null or weak positive associations. Some used proxy “traffic intensity” exposures (e.g. living near a busy road, home distance to a major road) in the analyses and reported null associations [11–13, 15]. In contrast, two studies found significant associations between self-reported traffic exposures near home and increased adult asthma prevalence [9, 10], but not when using individual modelled home outdoor NO2 or NOx (nitrogen oxides). Neither of these two studies examined NO2 or NOx effects on a continuous scale. A study of young adult Italians (aged 20–44 years) found that each 18.3 µg·m−3 increase of NO2 was nonsignificantly associated with increased asthma prevalence (OR 1.13, 95% CI 0.98–1.32) [10]. A national study among 12 177 Australian females reported a null association between 3-year mean annual NO2 and asthma prevalence [15].
In the SAPALDIA study, long-term exposure to PM10 was nonsignificantly associated with increased prevalence of current asthma (OR 1.19, 95% CI 0.83–1.70) in current smokers [14]. Recently, a study of 29 459 Canadian females reported that each 10 µg·m−3 increase of PM2.5 was significantly associated with increased ever-diagnosed asthma prevalence (OR 1.14, 95% CI 1.01–1.29). Association was stronger among smokers (OR 1.58, 95% CI 1.46–1.70) compared with nonsmokers (OR 1.16, 95% CI 0.96–1.41) [16].
A review of community-level studies in 2013 concluded that there was no evidence of an effect of long-term air pollution on asthma prevalence [6], although most of the studies included in that review were conducted in children (only two out of nine NO2 estimates and one out of nine PM10 estimates were for adults).
In contrast to most previous findings, our study suggests that both long-term PM10 and NO2 exposure is associated with increased lifetime asthma prevalence in adults. By pooling individual-level data from three large cohorts, our study has a much larger sample size and statistical power to detect an effect. Also, air pollution at the home address was modelled at a fine spatial scale (100 m grid) in our study, contributing to the observed robust associations.
Although findings in the prevalence studies were not entirely consistent, a positive association is increasingly suggested between ambient air pollution and incident asthma. In a nationwide cohort of US females, a borderline significant association between PM2.5 and incident asthma was observed (OR 1.20, 95% CI 0.99–1.46) [20]. However, this was not seen in the ESCAPE study (OR 1.04, 95% CI 0.88–1.23) [21]. Two studies reported significant associations between NO2 and incident asthma with similar effect sizes [17, 18]. In the ESCAPE study, NO2 was not associated with asthma incidence (OR 1.10, 95% CI 0.99–1.21) [21].
Effect estimates per 10 µg·m−3 were much larger for PM10 than for NO2. There are still debates on whether NO2 on its own causes health effects or merely is a marker of traffic-related, particularly near-road, air pollution [36]. Unlike NO2, particulate matter air pollution is more homogeneous over a wider region and includes sources other than traffic [37]. It was reported that in Europe, PM2.5 accounts for 40–80% of PM10 mass [29]. PM2.5, with various substances attached to it, could travel and deposit deep into the respiratory tract. These substances, including transitions metals and immunogenic substances, could either induce direct airway inflammation or lead to oxidative stress [5], i.e. two biological pathways linking to asthma. This may explain in part the relatively larger effect estimates seen for PM10.
A recent review concluded that no clear susceptibility factors could be identified to date for the link between outdoor air pollution and asthma incidence or prevalence [38]. One of the reasons, as the review suggested, may be that most studies lacked statistical power to perform interaction tests. In our study, due to the large sample size, we were able to investigate interactions among variables selected a priori. We found stronger associations among those aged ≥50 years, ever-smokers and less educated, adding evidence to the scant literature. The role of smoking status in the link between air pollution and asthma remains unclear. Some previous studies have reported stronger associations among never- and former-smoker [38] while two recent studies, including the ESCAPE study, observed an association only among ever-smokers [16, 21]. Different classifications of smoking status were used across previous studies, meaning results are not directly comparable. Smokers may have a higher risk of asthma [39] and it has been suggested that there may exist a synergistic effect of both tobacco smoking and air pollution exposure on asthma [40].
Asthma sufferers may move to less-polluted areas (e.g. far from a busy road) because of their illness, which could potentially lead to underestimation of the air pollution effects on adult asthma prevalence. However, in our study, mean duration of current residence was similar between subjects with asthma (16 years) and without asthma (16.7 years), and adjusting for residence years in Model 3 did not change the observed associations, suggesting migration is unlikely to have biased these associations.
Road traffic noise is rarely studied in relation to asthma morbidity. One study found that noise annoyance at night, as subjectively reported by 652 children, was significantly associated with asthma prevalence among girls [23]. Another study of 1383 middle-aged adults reported no association between frequency of intense traffic noise and current asthma prevalence [24]. Our much larger study did not find statistically significant associations between individual modelled noise exposure and ever-had asthma or current asthma prevalence, but data were not available to look directly at either asthma incidence or asthma exacerbations. It has been hypothesised that road traffic noise, as a psychological stressor, may induce alternations in the immune system, increase oxidative stress and disturb sleep, which all may potentially result in respiratory exacerbations, including asthma [41]. Increasing numbers of studies have linked other environmental stressors (e.g. neighbourhood violence, deprivation) to asthma morbidity [22], but more studies are needed to investigate the role of traffic noise on asthma.
Limitations
This study has a number of limitations. First, we adopted a cross-sectional design, which has limited value in establishing causal associations. Second, our asthma outcome was not strictly harmonised due to the wording of the original asthma question or variable recording of asthma-related medication data. Third, residual confounding cannot be ruled out as we were unable to harmonise other potential confounders and effect modifiers across the three cohorts, including environmental tobacco smoke, occupational exposures to gases and dust, family history of asthma and area-level socioeconomic status. Finally, the modelled air pollution and noise estimates inevitably had some exposure misclassifications, although this is unlikely to be differential according to the participant's asthmatic status. Given the broad geographic regions that this study covers, we adopted common LUR air pollution and noise models developed for Europe to minimise differences between cohorts that would otherwise be introduced by having different exposure assessment methods. This study is among the first to adapt the CNOSSOS-EU noise framework for epidemiological analysis; however, traffic flow data were not available for some secondary roads, which will lead to underestimation of noise levels in those areas. As with most air pollution and noise studies, we used home outdoor, but not indoor, air pollution and noise, which may be affected by building type and habits such as window opening, leading to further exposure misclassification.
Conclusions
In conclusion, this large cross-sectional study provides evidence suggesting that long-term ambient particulate air pollution, especially PM10, is associated with asthma prevalence in western European adults. No associations between traffic noise exposures and asthma prevalence were found. Our analyses were conducted using DataSHIELD, a novel “compute to the data” approach, which could help maximise the scientific potential of established cohorts by pooling personal data robustly yet ethically for research.
Acknowledgements
The Nord-Trøndelag Health Study (The HUNT Study) is a collaboration between the HUNT Research Centre (Faculty of Medicine, Norwegian University of Science and Technology NTNU), Nord-Trøndelag County Council, Central Norway Health Authority and Norwegian Institute of Public Health.
The authors wish to acknowledge the services of the Lifelines Cohort Study, the contributing research centres delivering data to LifeLines and all the study participants. This research was conducted using the UK Biobank Resource. We thank all study members and data collection teams of each biobank. We also thank Yannick Marcon (McGill University, Montreal, Canada), Chao Pang (University of Groningen, Groningen, The Netherlands), Eric Johnson, Federico Fabbri and Daniela Fecht (Imperial College London, London, UK), D2K team (Bristol University, Bristol, UK), and ESCAPE project (Utrecht University, Utrecht, The Netherlands) for their contributions to this work.
The views expressed are those of the authors and not necessarily those of the Dept of Health, the National Health Service or the National Institute for Health Research.
Author contributions are as follows. Concept and design: Y. Cai, S. Hodgson, M. Blangiardo, A.L. Hansell, P. Elliott. Writing of the paper: Y. Cai, P. Elliot, A.L. Hansell, S. Hodgson. Epidemiological data collection: K. Hveem, R.P. Stolk. Epidemiological data harmonisation: Y. Cai, D. Doiron, W.L. Zijlema, S. Mbatchou, I. Fortier. Air pollution and noise assessment: K. de Hoogh, D.W. Morley, J. Gulliver. Statistical analysis: Y. Cai, W.L. Zijlema, M. Blangiardo, A. Gaye, P.R. Burton. Discussion and interpretation of findings: Y. Cai, S. Hodgson, A.L. Hansell, M. Blangiardo, J. Gulliver, D.W. Morley, K. de Hoogh, P. Elliott. BioSHaRE Coordination Committee: I. Fortier, P.R. Burton, R.P. Stolk. All the authors revised the paper and approved the submission.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: The research leading to these results has received funding from the European Union Seventh Framework Programme (FP7/2007-2013) under grant agreement 261433 (Biobank Standardisation and Harmonisation for Research Excellence in the European Union (BioSHaRE)). BioSHaRE is engaged in a Bioresource Research Impact Factor (BRIF) policy pilot study (www.bioshare.eu/content/bioresource-impact-factor). DataSHIELD development is also partly funded under a strategic award from the UK Medical Research Council (MRC) and Wellcome Trust underpinning the ALSPAC (Avon Longitudinal Study of Parents and Children) project, and the Welsh and Scottish Farr Institutes funded by MRC, BBMRI-LPC (European Union Seventh Framework Programme: I3 grant). The Lifelines Cohort Study, and generation and management of genomewide association studies genotype data for the Lifelines Cohort Study, is supported by the Netherlands Organisation of Scientific Research NWO (grant 175.010.2007.006), the Economic Structure Enhancing Fund (FES) of the Dutch government, the Ministry of Economic Affairs, the Ministry of Education, Culture and Science, the Ministry for Health, Welfare and Sports, the Northern Netherlands Collaboration of Provinces (SNN), the Province of Groningen, University Medical Center Groningen, the University of Groningen, Dutch Kidney Foundation and Dutch Diabetes Research Foundation. Lifelines is a facility that is open for all researchers. Information on application and data access procedures is summarised at www.lifelines.nl. UK Biobank was established by the Wellcome Trust medical charity, MRC, Dept of Health, Scottish Government and the Northwest Regional Development Agency. It has also had funding from the Welsh Assembly Government, British Heart Foundation and Diabetes UK. The ESCAPE (European Study of Cohorts for Air Pollution Effects) project has received funding from the European Union Seventh Framework Programme (FP7/2007-2011) under grant agreement 211250. The MRC-PHE Centre for Environment and Health is funded by the MRC and Public Health England (PHE) (MR/L01341X/1). P. Elliott is a National Institute for Health Research (NIHR) Senior Investigator and acknowledges support from the Imperial College Healthcare National Health Service Trust and Imperial College London Biomedical Research Centre, the NIHR Health Protection Research Unit on the Health Effects of Environmental Hazards (HPRU-2012-10030-KCL), and the MRC-PHE Centre for Environment and Health. Funding information for this article has been deposited with the Open Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received December 16, 2015.
- Accepted September 1, 2016.
- Copyright ©ERS 2016
References










