





Abstract
Epidemiological data on late-onset noninfectious pulmonary complications (LONIPCs) following allogeneic haematopoietic stem cell transplantation (HSCT) are derived exclusively from retrospective studies and are conflicting. We aimed to evaluate prospectively the incidence, risk factors and outcomes for LONIPCs.
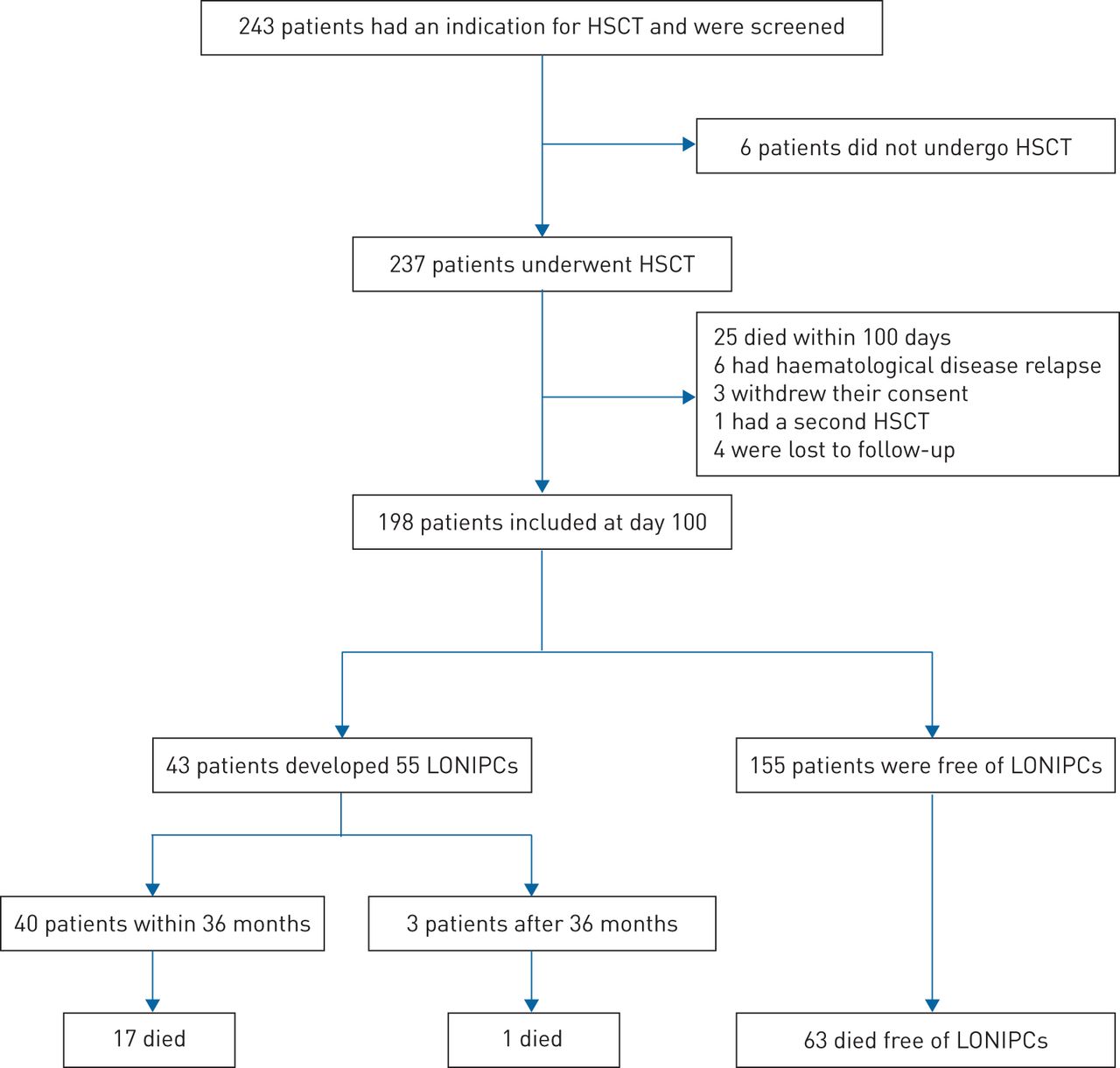
All consecutive patients scheduled to receive allogeneic HSCT between 2006 and 2008 at a university teaching hospital in France were screened for inclusion in the study. Eligible patients were those surviving at day 100. Among 243 screened patients, 198 patients were included in the analysis. The median (interquartile range) follow-up was 72.3 (15.2–88.5) months. 55 LONIPCs were diagnosed in 43 patients. Bronchiolitis obliterans syndrome (n=22) and interstitial lung disease (n=12) were the most common LONIPCs. At 36 months after inclusion, the estimated cumulative incidence of LONIPCs was 19.8% (95% CI 14.2–25.3%). The estimated median survival after the diagnosis of LONIPCs was 78.5 months (95% CI 20.0–not reached). Based on a multivariate Cox model, a history of chest irradiation anytime prior to HSCT, a history of pneumonia within 100 days post-HSCT and a low mean forced expiratory flow at 25–75% of forced vital capacity at day 100 were associated with the development of LONIPCs.
Our data provide clues to identify patients at high risk of developing LONIPCs. These patients should be targeted for close monitoring to provide earlier LONIPC treatment or prophylactic treatment.
Abstract
Chest irradiation, pneumonia and low FEF25–75% predict lung complications after allogeneic bone marrow transplantation http://ow.ly/pGel30j61Da
Introduction
Late-onset noninfectious pulmonary complications (LONIPCs) that occur beyond the third month following allogeneic haematopoietic stem cell transplantation (HSCT) have a significant effect on patient outcomes, with high associated mortality and morbidity rates [1–3]. Most of these lung complications that have been associated with chronic graft versus host disease (GVHD) mainly occur during the first year after HSCT and rarely occur beyond 2 years [3–6]. Although lung biopsy is the gold standard to classify most LONIPCs, fewer patients undergo lung biopsy, and the diagnosis mostly now relies on pulmonary function testing (PFT) and lung computed tomography (CT) scanning [7].
Findings from the available studies regarding both the incidence and risk factors for LONIPCs show many discrepancies. The reported incidence of LONIPCs ranges from 10% to 26% [1, 2, 7–11], while contradictory findings have been reported regarding the predictive role of the conditioning regimen, GVHD or stem cell sources [1–3, 7–11]. The main reason for these discrepancies is that all previous studies were retrospective, leading to significant biases, including incomplete data, an absence of detailed lung function and a lack of clinical correlation with most of the studies focused on PFT. In addition, most studies reviewed long periods characterised by variations in PFT screening strategies and diagnostic criteria for LONIPCs and HSCT procedures. Furthermore, although recommended, adherence to PFT guidelines in HSCT recipients is poor in routine practice and leads to missing data [12].
Specific limitations can be addressed for studies focused on bronchiolitis obliterans syndrome (BOS), which is the most frequent LONIPC. One of the main limitations is based on the difficulty in determining an accurate PFT definition for BOS to compare studies. Indeed, prior to the 2005 National Institutes of Health (NIH) consensus diagnostic criteria for BOS [13], various PFT criteria were used. Even after 2005, some authors used modified criteria to improve their sensitivity [4, 14, 15]. Recent studies have also shown that regardless of the diagnostic criteria of BOS, a significant proportion of patients experience a significant decline in forced expiratory volume in 1 s (FEV1) after HSCT [12]. Data suggest that this decline could be a good predictor for the development of subsequent BOS.
In addition to PFT, lung CT is an essential diagnostic tool for pulmonary complications. The evidence of air trapping by expiratory CT scan, small airway thickening or bronchiectasis are part of the BOS diagnostic criteria [15]. Whether any CT scan sign can predict the occurrence of post-HSCT BOS or other LONIPCs remains unknown.
Improved specification by LONIPCs and identification of early risk factors in a prospective study are mandatory to focus on high-risk allogeneic HSCT recipients to achieve an earlier diagnosis, initiate earlier treatment and evaluate prophylactic strategies to improve prognoses.
Methods
Study design and participants
In this observational prospective cohort study, all consecutive patients who were scheduled to receive an allogeneic HSCT between January 31, 2006 and December 31, 2008 at the Hôpital Saint-Louis (Paris, France) university teaching hospital were screened for inclusion within the 2 weeks before transplantation. Those allogeneic HSCT recipients surviving at day 100 in the absence of early relapse of haematological disease or refusal were included in the cohort. This study was approved by a central institutional review board (Comité Consultatif de Protection des Personnes dans la Recherche Biomédicale Paris Saint-Louis). All of the patients or legal guardians of the patients <18 years of age provided written informed consent before transplant, although definite inclusion occurred at day 100 after checking all inclusion and exclusion criteria. The trial was registered at ClinicalTrials.gov (identifier NCT01219972).
Procedures
At inclusion (day 100), the history of the underlying haematological disease, the characteristics of the transplant and the occurrence of GVHD in the first 100 days after HSCT were recorded.
PFT, lung high-resolution CT (HRCT) scans and a clinical assessment by a pulmonologist were performed sequentially before transplant, at inclusion, and then at 6, 12, 18, 24 and 36 months after HSCT. Thereafter, PFT was performed annually. Additional explorations were performed in the case of new-onset respiratory symptoms. PFT was performed using a body plethysmograph (Jaeger Masterscreen Body; CareFusion Germany 234, Hoechberg, Germany). Predictive values were determined as previously described [16]. As a pre-transplant lung function score (LFS) was previously associated with allogeneic HSCT recipient outcomes, LFS was determined [17].
HRCT scans were performed on every patient using a multislice CT scanner (Optima 660CT with low dose device; GE Healthcare, Milwaukee, WI, USA). Helicoidal acquisitions were acquired during both deep inspiration and expiration. The images were reconstructed using a high-spatial-frequency algorithm. One radiologist (C.d.M-M.) and two experienced pulmonary physicians (A.B. and K.C.) who were unaware of both the clinical and PFT results reviewed the CT scans and reached a conclusion by consensus. On the expiratory scans, the extent of air trapping was scored at three levels on axial images (upper, middle and lower) for each lung as: 1 (0–25% affected), 2 (25–50% affected), 3 (50–75% affected) or 4 (75–100% affected). For each lung, the score ranged from 6 to 24 [18, 19]. An air trapping score >6 was considered clinically significant.
End-points and definitions
Although previous studies suggested that LONIPCs mainly occur during the first year after HSCT and rarely occur beyond 2 years, in our clinical experience LONIPCs could occur beyond 2 years, particularly interstitial pneumonias. Therefore, in this prospective study, we decided to choose a follow-up of 36 months to obtain a further insight into such late occurrences by providing an estimate of occurrence over time within the first 3 years of HSCT. The main end-point was thus the occurrence of LONIPCs during the first 36 months following study inclusion. LONIPCs were classified as BOS, interstitial lung disease (ILD) and “others”, which included venous thromboembolic disease (VTED), air leak syndrome (i.e. pneumothorax or pneumomediastinum), exudative pleural effusion and restrictive lung defects (RLDs). Any LONIPC was considered during all of the follow-up, i.e. both at the time of planned CT scan or if diagnosed between two study visits. BOS was previously defined as: 1) an absence of respiratory infection at the time of PFT; 2) either an FEV1 <75% of predicted or a decline >10% of FEV1 from the pre-transplant value; and 3) either FEV1/vital capacity (VC) <0.7 or a concomitant decrease in both FEV1 and forced VC (FVC) <80% of predicted, with a total lung capacity (TLC) >80% of predicted [4, 20]. Concordance with the NIH definition was investigated for each case [13, 15]. These abnormalities persisted for two subsequent PFT measurements at 4-week intervals. A RLD was defined as a TLC <80% of predicted. ILD was diagnosed when diffuse opacities were present on HRCT and an infectious cause for these opacities was ruled out, as we reported previously [5]. VTED included pulmonary embolism diagnosed by CT pulmonary angiography or deep venous thrombosis diagnosed by ultrasound. Lower respiratory tract infection (LRTI) was defined as an association of fever, respiratory symptoms and a new lung infiltrate on chest radiography or lung CT scan. All these events were investigated with bronchoalveolar lavage, as described previously [5]. Proven LRTI was defined when a pathogen was documented. LRTI was defined as probable if clinical and radiological abnormalities improved with antimicrobial treatment but no pathogens were identified. Diagnostic criteria and severity of acute and extrathoracic chronic GVHD were assessed according to the NIH criteria, with a grading scale from 1 to 4 for acute GVHD [21], and the global score of mild, moderate and severe reflects the degree of organ impact and functional impairment due to chronic GVHD [15].
Secondary end-points were survival after LONIPCs and long-term time course of PFT (FEV1, FVC, TLC, mean forced expiratory flow (FEF) at 25–75% of FVC (FEF25–75%) and instantaneous FEF at 50% of FVC (FEF50%)). For descriptive purposes, overall survival was also computed.
Statistical analysis
Summary statistics were reported, i.e. median (interquartile range (IQR)), unless otherwise stated. All analyses of survival data were performed using data obtained up to June 2016.
Survival after inclusion (day 100 after HSCT) and survival after LONIPCs were both estimated using the Kaplan–Meier method; a Cox model with a time-dependent variable was used to assess the impact of LONIPCs on survival. Competing-risk end-points (LONIPC, BOS, chronic GVHD and relapse) were computed from study inclusion in which patients who died free from the event of interest were considered competing-risk events. Early risk factors were defined as those present before transplantation or at inclusion (day 100). Predictive analyses of the hazard of LONIPC or BOS occurrence within the first 36 months were based on cause-specific Cox models. First, univariate models were fitted whereby all the covariates reported previously as risk factors for LONIPCs were considered fixed covariates; chronic GVHD after inclusion was tested as a time-dependent covariate. Then, multivariate models were fitted on those predictors selected from univariate analyses at the 10% level, segregating pre-transplant, transplant and post-transplant (at day 100) characteristics. Finally, multivariate models were fitted based on all potential predictors selected whatever the time of measurement at the 10% level, with model selection based on a stepwise procedure using variables associated with the outcome at the 5% level and after multiple imputations with chained equations (MICE) of missing data, averaging the estimates over 50 data sets. Sensitivity analyses based on a complete case analysis were also performed.
To describe the course of PFT over time, we used a nonparametric k-means algorithm for clustering longitudinal data, providing several techniques for dealing with missing values in trajectories; the number of trajectories was defined as those maximising the Calinski–Harabatz criterion as given by the kml package [22]. All estimates of cumulative incidence, survival rates and cause-specific hazard ratios were reported with 95% confidence intervals.
Statistical analyses were performed using SAS version 9.3 (SAS Institute, Cary, NC, USA) and R version 3.2.2 (www.R-project.org). Two-sided p-values ≤0.05 indicated statistical significance.
Results
From May 2006 to April 2009, 198 out of 243 screened patients were included in the analysis (figure 1). Two (1%) patients had FEV1/VC <0.7 and nine (5%) patients had a RLD. LFS was impaired in 118 (75%) patients. 35 (23%) patients had a significant air trapping score (>6) on chest CT scan. Pre-transplantation and inclusion data (day 100) are summarised in table 1.

Study flowchart. HSCT: haematopoietic stem cell transplantation; LONIPC: late-onset noninfectious pulmonary complication.
Patient characteristics measured before or at the time of allogeneic haematopoietic stem cell transplantation (HSCT) and at the time of inclusion (day 100 after allogeneic HSCT)
Within 100 days following HSCT, 33 (17%) patients developed grade ≥3 acute GVHD (skin, n=31; liver, n=7; gut, n=19) and 11 (6%) patients had extensive chronic GVHD. Nine of the 18 LRTIs were documented (bacteria, n=3; fungus, n=2; virus, n=4). There were no notable differences between the patients included and not included in the study (supplementary table S1).
The median (IQR) duration of follow-up was 72.3 (15.2–88.5) months. Three patients were lost to follow-up at 5, 14 and 28 months, respectively; 40 patients relapsed; and 81 patients died (48 free of relapse and 33 after relapse), 68 within 36 months, with a 3-year survival of 65.4% (95% CI 59.1–72.4%) (figure 2a). In addition to relapse, patients died mostly from pulmonary causes (n=18; 14 due to infectious pneumonia and four from respiratory failure), 16 from GVHD, seven from other causes, while 11 causes of death were unknown.

Estimated survival of allogeneic haematopoietic stem cell transplantation recipients included in the cohort (100 days after transplantation): a) overall survival (95% CI) whatever the cause of death and b) cumulative incidence of deaths according to cause. GVHD: graft versus host disease.
55 episodes of LONIPCs were diagnosed in 43 patients (figure 1). Diagnoses included BOS (n=22 in 22 patients), ILD (n=12 in 12 patients) and others (n=21 in 19 patients). LONIPCs other than BOS and ILD included various diagnoses (table 2). 10 patients developed more than one LONIPC (BOS and ILD, n=2; RLD and ILD, n=1; BOS and VTED, n=1; pleural effusion and VTED, n=1; VTED and ILD, n=1; BOS and RLD, n=2; BOS and ILD and pneumothorax, n=1; BOS, pneumothorax and VTED, n=1).
Diagnoses of late-onset noninfectious pulmonary complications (LONIPCs) observed in the sample
Most of the patients (39 out of 43 (91%)) developed the first episode of LONIPC within 36 months (figure 3). At that time, the estimated cumulative incidence of LONIPCs was 19.8% (95% CI 14.2–25.3%). All 22 episodes of BOS occurred within 36 months, with an observed median (IQR) time of 8.8 (2.9–19.7) months after inclusion. The cumulative incidence of BOS at 36 months was 10.7% (95% CI 6.3–15.1%) (figure 3). Of the 22 BOS episodes, 20 (91%) fulfilled the NIH criteria, either at the same time (n=8) or subsequently within a median (IQR) time of 106 (17–128) days (n=12).

Cumulative incidence of late-onset noninfectious pulmonary complications (LONIPCs), overall and segregated into bronchiolitis obliterans syndrome (BOS), interstitial lung disease (ILD) and others.
We evaluated early predictive factors for LONIPCs diagnosed in the first 36 months after HSCT; factors selected by univariate analyses are presented in table 3.
Predictive factors for the development of bronchiolitis obliterans syndrome (BOS) and late-onset noninfectious pulmonary complications (LONIPCs) during the first 3 months after haematopoietic stem cell transplantation (HSCT): results of univariate and multivariate analyses
Multivariate models were fitted based on pre-transplant, transplant and post-transplant characteristics, separately (table 3). They exhibit the summarised predictive value of sex and history of chest irradiation before transplant, of human leukocyte antigen-related donor at transplant, and of the occurrence of a LRTI within 100 days post-transplant.
Based on multivariate Cox models that included all previously selected predictors, pre-transplant chest irradiation, LRTI before inclusion and low FEF25–75% at inclusion were jointly associated with the occurrence of LONIPCs (table 4). Similar results were obtained for a complete case analysis.
Predictive factors for the development bronchiolitis obliterans syndrome (BOS) and late-onset noninfectious pulmonary complications (LONIPCs) during the first 3 months after haematopoietic stem cell transplantation (HSCT): results of multivariate analyses
We re-evaluated these predictors to predict BOS (table 3). Multivariate models selected the use of peripheral blood stem cells and bronchial abnormalities on the CT scan (including centrilobular micronodules, tree-in-bud pattern and bronchial thickening) at inclusion as associated with the occurrence of BOS. Based on a complete case analysis, LRTI and a 10% FEV1 decline from baseline to day 100 were selected instead of bronchial abnormalities (table 4).
We further investigated whether the occurrence of chronic GVHD after inclusion (i.e. any time during the whole follow-up from day 100 and before the LONIPC) was predictive of LONIPCs/BOS. The cause-specific hazard of LONIPCs was increased by 2.25 (95% CI 1.07–4.75; p=0.03) after the occurrence of a chronic GVHD; that of BOS was increased by 2.90 (95% CI 0.98–8.60; p=0.05).
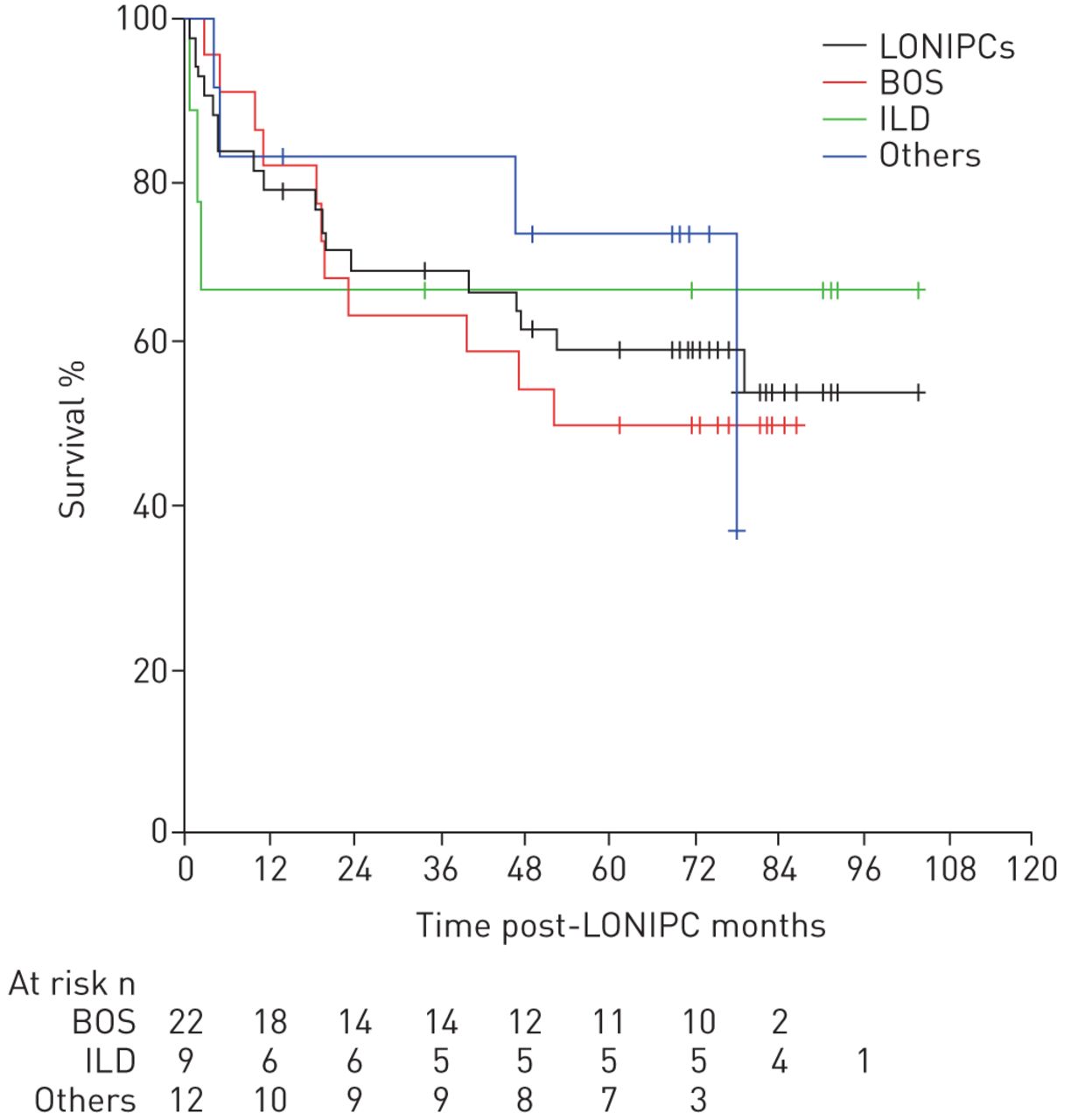
Among the 43 patients with LONIPCs, 18 died (nine after BOS, three after ILD, two after VTED, two after RLD, one after both BOS and RLD, and one after pneumomediastinum, BOS and ILD), with a median survival after diagnosis of 78.5 months (95% CI 20.0–not reached). At 3 years after BOS, survival was 63.6% (95% CI 46.4–87.3%) (figure 4). The occurrence of LONIPCs was associated with an increased hazard of death (HR 2.18, 95% CI 1.14–4.15; p=0.02).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Overall survival after late-onset noninfectious pulmonary complications (LONIPCs), overall and segregated into bronchiolitis obliterans syndrome (BOS), interstitial lung disease (ILD) and others.
At the end of follow-up (i.e. 100 months), almost 80% of the patients presented a significant PFT decrease at least once, particularly a 10% decline in FEV1 (supplementary figure S1). As depicted in supplementary figure S2, all patients who were free from LONIPCs had roughly stable FEV1 values over time, regardless of their baseline value. In contrast, the FEV1 trajectories differed among patients with BOS with two different clusters (supplementary figure S3).
Discussion
We confirmed prospectively that LONIPCs are frequent complications that largely occurred within 2 years after allogeneic HSCT with a poor outcome. Although BOS accounted for more than half of LONIPCs, these complications included heterogeneous entities, demonstrating that the risk factors for LONIPCs and BOS are distinct.
Most of the variables that we tested as risk factors have previously been associated with LONIPCs or BOS in one or more previous retrospective studies, with contradictory conclusions. As the procedures applied for allogeneic HSCT change over time, including conditioning regimens and stem cell sources, the evaluated risk factors for LONIPCs have evolved over time. Some studies have proposed that chronic GVHD is a risk factor for BOS [6, 23]. Due to the retrospective design of these studies, we wondered whether chronic GVHD was contemporaneous to LONIPCs/BOS rather than a predictive risk factor. As expected, few patients developed chronic GVHD within 100 days following transplantation. However, prolonged follow-up of our patients led us to conclude that chronic GVHD was actually associated with the occurrence of LONIPCs. The physiopathological hypotheses of LONIPCs/BOS is that lung injury caused by various insults could be the trigger for an uncontrolled inflammatory reaction, leading to aberrant tissue repair [24]. We found that a history of chest irradiation and the occurrence of early pneumonia after HSCT were strongly predictive of LONIPCs/BOS, reinforcing this hypothesis.
The diagnosis of post-transplant BOS using noninvasive methods is challenging [24]. In the early 2000s, lung CT emerged as a promising tool to diagnose BOS [25, 26]. Some authors have even suggested that the presence of air trapping on expiratory scans could precede PFT impairment [27, 28]. These data led to the inclusion of air trapping as a diagnostic criterion for post-allogeneic HSCT BOS in the NIH consensus [13, 15]. We were surprised to find that nearly a quarter of patients had significant air trapping before transplantation. This phenomenon could be attributed to the observation that allogeneic HSCT recipients are older and have a history of respiratory events explaining the air trapping, including respiratory infection during a prior course of chemoradiotherapy. Furthermore, although the proportion of patients with significant air trapping increased at day 100 after transplant, air trapping was not predictive of BOS. Conversely to air trapping, bronchial abnormalities at day 100, including centrilobular micronodules, tree-in-bud pattern and bronchial thickening, were predictive of BOS. This finding is of particular interest because these CT scan abnormalities could reflect the early phase of inflammatory bronchiolitis obliterans when treatment could be effective.
To date, PFT is the cornerstone of BOS diagnosis [15]. However, the current criteria do not allow for consideration of all BOS [4, 29, 30]. Recently, Thompson et al. [3] showed that the median change in FEV1 from pre-transplant to day 100 in patients who subsequently developed LONIPCs was significantly greater than that in unaffected patients. We found that a decrease in airflow at day 100, both in proximal and small airways (i.e. FEV1 and FEF), was predictive of LONIPCs/BOS. In particular, a 10% decline in FEV1 from pre-transplant to day 100 was predictive of BOS in the multivariate analysis. These findings strongly encourage monitoring spirometry early after an allogeneic HSCT and suggest consideration of the trajectory of FEV1 rather than the absolute value at a given time. This finding is consistent with the findings of Cheng et al. [31], who observed a rapid FEV1 decline during the 6 months prior to BOS diagnosis.
Our prospective cohort provides a unique opportunity to assess allogeneic HSCT recipient lung function over a long follow-up period. Thus, we have shown that lung function fluctuated and that a very significant proportion of patients experienced a significant decline in airflow at least once during their follow-up. However, FEV1 or FEF mostly returned to baseline values in the follow-up PFT. The many events that occur after transplant can explain this issue, especially respiratory infections and a transient deterioration in the general condition that jeopardises the quality of spirometric performance.
Finally, we provide important data regarding BOS. We used a definition that differs from that of the NIH consensus, which allowed an earlier diagnosis of BOS. Of note, we used this definition in previous studies [4, 20]. In addition, we identified two phenotypes of BOS according to the trajectory of FEV1 with different outcomes. This result raises the question of a different pathophysiological mechanism and whether different approaches for management should be investigated.
Our study has several limitations. First, due to the small number of patients who experienced LONIPCs other than BOS, we could not reliably evaluate the risk factors for each specific LONIPC. Second, our study was a single-centre study; however, given that all PFT was performed at the same place using the same plethysmograph, this reinforces the value of our PFT variations findings by reducing inaccuracy and avoiding potential bias incurred by PFT performed using different machines. Nevertheless, the single-centre recruitment limits the external validity required to support widespread changes in practice; results should thus apply at the bedside only after comparing the context of the study with the context of clinical experience. Third, some data were missing, especially some PFT and CT scans during forced expiration, which were difficult to obtain in patients with poor general health. However, missing data were imputed with no main modifications of the results. Indeed, the various predictive factors for BOS that were identified either after multiple imputation (MICE) or multivariate analysis of the complete cases were actually correlated (data not shown). Finally, we did not collect data to allow calculating scores that were shown to be independently predictive of increased mortality after allogeneic HSCT, such as the haematopoietic cell transplantation-specific comorbidity index or the disease risk index [32, 33]. Thus, this issue precluded their assessment in our predictive models for LONIPCs. This could be explored in further studies.
In conclusion, our data provide clues to identify patients with a high risk of developing LONIPCs. These patients should be targeted for close monitoring, especially PFT, and thus offered earlier treatment of LONIPCs or prophylactic treatment to improve outcomes.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02617-2017_Supplement
Acknowledgements
The authors thank Stéphane Cassonnet and Emmanuelle Bugnet (Hôpital Saint-Louis, Paris, France) for the clinical study coordination and technical support, Nathalie Chemla and Stéphane Beziaud (Clinique du Sport, Paris, France) for performing the lung CT scans, Françoise Grondin (Hôpital Saint-Louis) for performing the pulmonary function tests, and Elisabeth Savariau (Hôpital Saint-Louis) for excellent technical assistance. We also thank all HSCT recipients who participated in the study and EGMOS, an association of bone marrow transplant recipients. In memory of Laurène, an allogeneic HSCT recipient, for her energy, her help and her strong desire to advance research on LONIPCs.
Footnotes
This article has supplementary material available from erj.ersjournals.com
This study is registered at ClinicalTrials.gov with identifier number NCT01219972.
Conflict of interest: A. Bergeron has received personal fees for lectures from Gilead and Pfizer, and personal fees for lectures and board participation from Merck, outside the submitted work. R. Peffault de Latour has received personal fees and grants from Alexion, Novartis and Pfizer, and research grants from Amgen, outside the submitted work. K. Chagnon has received personal fees from AstraZeneca, outside the submitted work.
Support statement: This study was supported by an institutional grant from the French Ministry of Health (CRC 04118), which had no role in the study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to the data in the study and the final responsibility for the decision to submit the study findings for publication.
- Received April 19, 2017.
- Accepted March 14, 2018.
- Copyright ©ERS 2018
References










