





Abstract
We aimed to describe the differences and similarities between patients with chronic obstructive airway disease classified on the basis of classical diagnostic labels (asthma, chronic obstructive pulmonary disease (COPD), or asthma–COPD overlap (ACOS)) or according to the underlying inflammatory pattern (Th-2 signature, either Th-2-high or Th-2-low).
We performed a cross-sectional study of patients aged ≥40 years and with a post-bronchodilator forced expiratory volume in 1 s to forced vital capacity ratio ≤0.7 with a previous diagnosis of asthma (non-smoking asthmatics (NSA)), COPD or ACOS, the latter including both smoking asthmatics (SA) and patients with eosinophilic COPD (COPD-e). Clinical, functional and inflammatory parameters (blood eosinophil count, IgE and exhaled nitric oxide fraction (FeNO)) were compared between groups. Th-2 signature was defined by a blood eosinophil count ≥300 cells·μL−1 and/or a sputum eosinophil count ≥3%.
Overall, 292 patients were included in the study: 89 with COPD, 94 NSA and 109 with ACOS (44 SA and 65 with COPD-e). No differences in symptoms or exacerbation rate were found between the three groups. With regards the underlying inflammatory pattern, 94 patients (32.2%) were characterised as Th-2-high and 198 (67.8%) as Th-2-low. The Th-2 signature was found in 49% of NSA, 3.3% of patients with COPD, 30% of SA and 49.3% of patients with COPD-e. This classification yielded significant differences in demographic, functional and inflammatory characteristics.
We conclude that a classification based upon the inflammatory profile, irrespective of the taxonomy, provides a more clear distinction of patients with chronic obstructive airway disease.
Abstract
Identifying a Th-2 signature in patients with chronic airflow limitation effectively differentiates treatable traits http://ow.ly/kq1E309MMkt
Introduction
Asthma and chronic obstructive pulmonary disease (COPD) are two common diseases in the general population that occasionally may share similar clinical features and physiopathological mechanisms [1, 2]. Irrespective of whether or not asthma and COPD share a common origin, they are both heterogeneous conditions that can present with a wide range of clinically overlapping pictures, commonly labelled as phenotypes. However, this approach does not take into account the growing knowledge about molecular pathways (i.e. endotypes) that has allowed novel therapeutic strategies to be developed that target specific components of the underlying inflammatory process. As a consequence, some experts have proposed to move to a precision medicine scenario that takes into consideration causal mechanistic disease pathways in order to plan treatment according to “treatable traits”, specific for each patient [3]. So far, only markers of Th-2 inflammation (e.g. sputum or blood eosinophil counts, exhaled nitric oxide, periostin, IgE) have been incorporated into the diagnostic and therapeutic process for patients with chronic obstructive airway disease (COAD). Current evidence suggests that eosinophilia is associated with COPD treatment response and natural history [4, 5]. Moreover, a Th-2 signature in smokers and ex-smokers with COPD is associated with an increased blood eosinophil count, bronchial hyper-responsiveness and a response to inhaled corticosteroids (ICS) that is not predicted by a previous history of asthma [6]. The classification of asthmatic patients based on their inflammatory pattern (namely “Th-2-high” and “Th-2-low”) has allowed the development of new biological agents [7].
The so-called asthma–COPD overlap syndrome (ACOS) has recently gained attention but, to date, there is no universally accepted definition of this entity though some efforts have been undertaken to characterise it [8–11]. One of the reasons for this confusion might be that all the clinical studies carried out to describe ACOS have included selected cohorts of patients with asthma or COPD instead of considering COAD as a whole. Such an approach is clearly inadequate to address some important clinical questions, such as, to what extent are COPD with eosinophilia and asthma with chronic airflow limitation in smokers the same entity.
The objective of this study was to describe the demographic, clinical and physiological differences and similarities between patients with COAD classified either on the basis of classical diagnostic labels (asthma in non-smoking asthmatics (NSA), COPD or ACOS, the latter including smoking asthmatics (SA) and patients with eosinophilic COPD (COPD-e)) or according to the underlying inflammatory pattern (Th-2 high and Th-2 low). As a secondary objective, we aimed to explore how the new proposed criteria to define ACOS [9] fit into the different categories.
Material and methods
Study design
We carried out a cross-sectional, observational, multicentre study in 23 outpatient clinics based in tertiary hospitals in Spain run by expert respiratory physicians. Investigators were asked to recruit consecutive patients with asthma, including smoking and non-smoking patients and patients with COPD with and without a blood eosinophil count ≥200 eosinophils·μL−1.
The study was approved by the Research Ethics Committee of the Balearic Islands (Cod: IB2499/15). Additionally, an independent ethics committee or institutional review board for each study centre approved the final protocol. The STROBE standards (STrengthening the Reporting of OBservational studies in Epidemiology) for reporting observational studies were followed.
Patients
We included male and female patients aged ≥40 years with a history of physician-diagnosed asthma or COPD (as defined below) and chronic airflow obstruction (a post-bronchodilator forced expiratory volume in 1 s (FEV1) to forced vital capacity (FVC) ratio ≤0.70) who signed an informed, written consent form. Patients had to be in a stable condition, free from exacerbations for at least 3 months. Exclusion criteria included primary bronchiectasis, active cancer (metastatic, progressive or treated within the last 24 months), chronic inflammatory diseases and a poor performance status. Active smoking was not an exclusion criterion.
Definitions
-Non-smoking asthmatics (NSA): patients with a history of physician-diagnosed asthma according to international guidelines [8], with chronic airflow obstruction, who were either never-smokers or ex-smokers with a smoking history of ≤10 pack-years.
-Smoking asthmatics (SA): asthma patients with chronic airflow obstruction and a smoking history of ≥20 pack-years.
-COPD: diagnosed according to international recommendations [2] by the presence of a post-bronchodilator FEV1/FVC ≤0.70 in patients with a smoking history of ≥10 pack-years in the absence of clinical suspicion for asthma.
-COPD with eosinophilia (COPD-e): COPD patients with an eosinophil count ≥200 eosinophils·μL−1 in blood. We selected this threshold because below this cut-off patients are unlikely to have sputum eosinophilia, according to published evidence [12].
-ACOS: We considered this diagnosis if the patient, previously diagnosed with asthma, had chronic airflow limitation and a smoking history ≥20 pack-years, or if a patient with a diagnosis of COPD had a blood eosinophil count ≥200 eosinophils·μL−1. We also tested in our population the validity of the latest expert consensus definition of ACOS [9], which is the presence of chronic airflow limitation (a post-bronchodilator FEV1/FVC ≤0.7) in patients ≥40 years with a smoking history of ≥10 pack-years and a documented history of asthma or a large bronchodilator response (defined by an increase in FEV1 ≥400 mL and ≥15%) in whom one of the following characteristics is present: history of atopy or allergic rhinitis, blood eosinophil count ≥300 cells·μL−1 or a bronchodilator response (increase in FEV1 ≥200 mL and 12%) in two or more visits.
-COAD with Th-2-high: Patients with a post-bronchodilator FEV1/FVC ≤0.70 and an eosinophil count ≥300 eosinophils·μL−1 in blood or ≥3% in sputum.
-COAD with Th-2-low: Patients with a post-bronchodilator FEV1/FVC ≤0.70 and an eosinophil count ≤300 eosinophils·μL−1 in blood and ≤3% in sputum.
-Exacerbation: Sustained worsening of the patient's condition, sufficient to warrant treatment with antibiotic or oral corticosteroid therapy or admission to hospital. Each episode must have been recorded in the medical chart.
Measurements
The study was conducted in a single visit in which the researchers obtained and recorded all the clinical data into an electronic clinical research database. A blood sample was obtained to determine the number and percentage of blood eosinophils and to quantify the level of IgE. Atopy was assessed by a skin prick test. The degree of compliance with inhalers was estimated using the Test of Adherence to Inhalers [13].
Pulmonary function tests and measurement of the exhaled nitric oxide fraction (FeNO) were performed following American Thoracic Society (ATS)/European Respiratory Society (ERS) guidelines [14–16].
Sputum induction was performed in 32 patients, in selected centres, according to the ERS recommendations [17]. We adopted a sputum eosinophil count of 3% as the threshold for defining eosinophilic or non-eosinophilic airway inflammation, as described elsewhere [18].
Statistical analysis
Data are summarised as relative frequencies for categorical variables, mean±sd for normally distributed scale variables, and frequency and percentage for ordinal or non-normal scale variables. To compare differences between groups, an ANOVA or Kruskal–Wallis test was used for parametric continuous or nonparametric continuous variables, respectively. To compare categorical variables, a Pearson's Chi-squared test or Fisher's exact test (when applicable) was used. The Bonferroni correction was used to control for type I errors. The significance level was established as a two-tailed p-value <0.05.
Results
Population characteristics
In total, 292 patients with COAD were included in the study (figure 1): 94 NSA, 89 with COPD and 109 with ACOS (44 SA and 65 with COPD-e). The demographic, clinical and functional characteristics of the entire sample are reported in table 1. Briefly, the degree of bronchial obstruction was moderate and symptoms were fairly controlled as assessed by the COPD Assessment Test (CAT) and Asthma Control Test (ACT) questionnaires. The average number of exacerbations in the course of the previous 12 months was 1.0±1.35. Most patients (80%) were treated with ICS and almost all of them received a long-acting β2-agonist (LABA). About 71% were being treated with a long-acting muscarinic antagonist (LAMA) (table 1). Corrected post hoc p-values for two-group comparisons are shown in supplemental table S1.

Flow-chart diagram of recruitment process. FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; COPD: chronic obstructive pulmonary disease; ACOS: asthma–COPD overlap syndrome.
Characteristics of patients according to the baseline diagnosis
Characteristics of patients with chronic obstructive airway disease according to current taxonomy
NSA patients were middle-aged (61.1±12.3 years), predominantly female, with frequent symptoms of rhinitis (53%) and the most preserved pulmonary function (mean post-bronchodilator FEV1: 69.5±18.9% of reference value). They showed the highest values for blood eosinophil count, FeNO, and IgE (table 1). Virtually all of these patients were receiving a combination of ICS with LABA and >50% were also treated with LAMA as an add-on therapy. About 17% were on omalizumab, whereas only 6.4% were receiving oral corticosteroids (table 1). Within the previous year, 47% had at least one exacerbation. The mean number of exacerbations in the previous year was 0.97±1.37. In this group, none of the patients met the consensus criteria for ACOS.
COPD patients were older (67.9±8.6 years), predominantly male, and had the most severe airflow limitation (mean post-bronchodilator FEV1: 55.1±18.5%; diffusing capacity of the lung for carbon monoxide (DLCO): 63.6±25.9) and the highest smoking history. This group also had the lowest values for blood eosinophil count, FeNO and IgE among the three groups (table 1). The majority of these patients were being treated with a combination of LABA and LAMA but 66% of them were also receiving ICS (table 1). Within the previous year, 52% had at least one exacerbation. The mean number of exacerbations in the previous year was 1.08±1.32. In this group, 5.6% of the patients met the consensus criteria for ACOS. None of them had a previous history of asthma but all had a high response to bronchodilation plus a history of atopy.
Characteristics of patients with chronic obstructive airway disease included in the category of asthma−COPD overlap syndrome
The ACOS category included 109 patients (44 SA and 65 COPD-e). When compared with the NSA and COPD patients, we found no differences in symptoms or exacerbations. ACOS patients showed similar demographic and inflammatory characteristics to those with asthma and functional impairment and a comorbidity profile similar to those in the COPD group (table 1). About 75% of these patients were taking ICS regularly, almost all of them (93%) were receiving a LABA, 73% were treated with a LAMA and 8.6% were on omalizumab treatment (table 1). In this category, 38.5% of the patients met the consensus criteria for ACOS [9]. The patients who met the consensus criteria for ACOS were younger and had a lower smoking history, a more frequent history of rhinitis and better lung function than those considered to have ACOS according to our definitions (supplemental table S2).
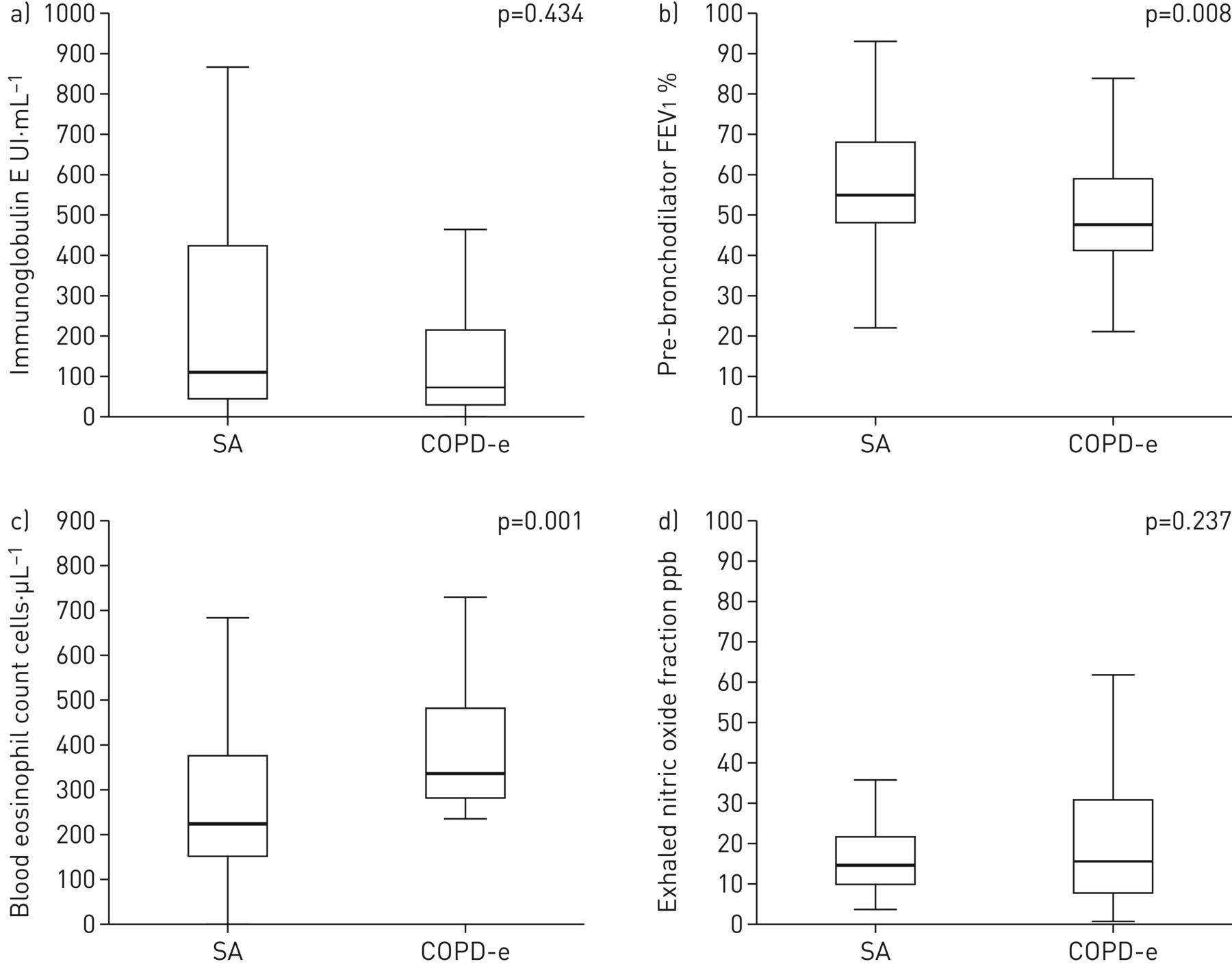
There were important differences between patients included in the category of ACOS depending on whether the patient had a diagnosis of SA or of COPD-e (table 2 and figure 2). Patients classified with COPD-e showed significantly lower post-bronchodilator FEV1 than SA patients (54.49±15.2 versus 65.57±17.5%; p=0.005), but a higher blood eosinophil count (374.9±156 versus 262.1±189 cells·μL−1, p<0.002) and a non-statistically significant trend for higher FeNO values (24.6±25.4 versus 19.6±11 ppb, p=0.237) than those found in the SA group.
Differential characteristics within the asthma–COPD overlap syndrome group: smoking asthmatics versus eosinophilic COPD

Differential characteristics within the asthma–chronic obstructive pulmonary disease overlap syndrome group: smoking asthmatics (SA) versus eosinophilic COPD (COPD-e). FEV1: forced expiratory volume in 1 s.
The SA group showed similar demographic and functional characteristics to those in the NSA group, with frequent symptoms of rhinitis (51%) and positive results in skin prick tests (45.5%). However, blood eosinophil count and FeNO values were lower than those found in the NSA group (262.1±189 versus 395.5±505 cells·μL−1, p<0.001 and 19.6±17 versus 36.0±27 ppb, p<0.001, respectively). The therapeutic approach was similar in NSA and SA. In the previous year, 52% of patients had at least one exacerbation. The mean number of exacerbations in the previous year was 1.00±1.36. In this subgroup, 77.3% of the patients met the consensus criteria for ACOS. Those patients who did not meet the criteria had a previous diagnosis of asthma but did not meet any of the minor criteria to be considered under ACOS: no atopy, no rhinitis, no bronchodilator response and no eosinophil count ≥300 cells·μL−1.
Patients with COPD-e showed similar smoking habits and demographic and functional characteristics to those in the COPD category with the exception of more reversibility of the airflow obstruction (positive bronchodilator test 30.2% versus 19.2%). However, although the blood eosinophil counts were higher than those found in the COPD group (374.9±156 versus 118.2±63 cells·μL−1, p<0.001), differences in FeNO values did not reach statistical significance (24.6±25.4 versus 17.3±9.6 ppb, p>0.05). The therapeutic regimen was similar to that in the COPD group. In the previous year, 49% of patients had at least one exacerbation. The mean number of exacerbations in the previous year was 0.95±1.37. In this subgroup, 12.3% met the consensus criteria for ACOS. None of them had a previous history of asthma but had a high bronchodilator response plus atopy, rhinitis or a blood eosinophil count ≥300 cells·µL−1.
Characteristics of patients with chronic obstructive airway disease according to the underlying inflammatory profile
Out of the 292 patients included in the study, 94 (32.2%) were characterised as Th-2-high and 198 as Th-2-low. Th-2 signature was found in 49% of NSA, 3.3% of patients with COPD, 30% of SA and 49.3% of patients with COPD-e (figure 3). The criteria for ACOS was met by 22% of patients categorised as Th-2-high and 18.7% of patients categorised as Th-2-low.

Proportional squares showing the percentage Th-2 signature in patients with chronic obstructive pulmonary disease (COPD), asthma, or asthma–COPD overlap syndrome (ACOS), the latter comprising smoking asthmatics (SA) and patients with eosinophilic COPD (COPD-e).
Th-2-high patients were significantly younger (60.9±12.3 versus 65.8±9.8 years; p=0.003) with a longer history of symptoms (age of onset: 41.0±19.1 versus 50.5±18.0 years; p<0.001). No gender differences were seen between groups. Th-2-high patients had a more frequently positive skin prick test (46.8% versus 21.2%; p<0.01) as well as more frequent rhinitis (55.5% versus 22.8%; p<0.001) and polyposis (24.7% versus 4.9%; p<0.001). Pulmonary function was significantly better in Th-2-high patients (post-bronchodilator FEV1: 1779±751 versus 1593±697 mL, p=0.01). There were no differences in the total number of exacerbations (2.2±1.5 versus 1.8±1.1; p= 0.18) or in symptoms assessed by CAT (14.3±8 versus 13.3±7; p=0.38) and ACT (19.4±4 versus 20.2±4; p=0.28) questionnaires. Th-2-high patients had more corticosteroid-treated exacerbations (0.97±1.46 versus 0.57±0.97; p=0.057). Th-2 biomarkers were significantly higher in Th-2-high patients, including blood eosinophil count (median 450 versus 180 cells·µL−1; p<0.01), IgE (median 143 versus 64 UI·mL−1; p<0.001) and FeNO (median 28 versus 15 ppb; p<0.001) (table 3 and figure 4).
Differential characteristics according to the baseline inflammatory pattern

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Differential characteristics according to the baseline inflammatory pattern. FEV1: forced expiratory volume in 1 s.
No differences were found between the two groups in the percentages of patients who were taking ICS, LABA, LAMA, oral corticosteroids and omalizumab (table 3).
Discussion
We have shown that the current distinction between asthma, COPD and their overlap (ACOS) may be confusing because it includes a variety of disease expressions that cannot be separated clinically, and that a view of COAD based on the presence of a Th-2 signature is feasible and more effective for identifying treatable traits.
Patients with COPD and NSA patients with chronic airway obstruction share common symptoms, but they can be distinguished based on demographic, atopic and functional features. However, ACOS manifestations are somewhere between COPD and asthma, given that these patients showed analogous demographic and inflammatory characteristics to those with asthma, as well as functional impairment and comorbidities similar to those included in the COPD group. If we apply the criteria proposed by an expert panel [9] to identify ACOS patients, we could classify in this category 11.7% of the NSA patients, 5.6% of the COPD patients, 77.3% of the SA patients and 12.3% of the COPD-e patients. Therefore, these criteria mainly identify as ACOS asthmatic patients who have smoked and developed a “fixed bronchial obstruction”, but also a non-negligible number of patients diagnosed with COPD or asthma by their physicians. If we consider ACOS as the coincidence of two different diseases (asthma and COPD) in the same individual, we should expect a mixed inflammatory pattern with some “Th-2-high” expression, and this situation might occur in both SA and COPD-e patients. However, we found significant differences between these two subgroups: SA patients had similar demographic and functional characteristics as NSA patients, but only 30% of them showed a Th-2-high inflammatory pattern (versus 49% in the NSA group). COPD-e patients had similar demographic and functional features as patients with “pure COPD”, but the proportion of patients with a Th-2-high inflammatory pattern (49.3%) was almost identical to that observed in NSA. Therefore, the “historic classification” does not reflect the inflammatory heterogeneity that exists behind COAD.
Previous attempts to cluster patients with both asthma and chronic airflow obstruction and COPD identified patients with severe and markedly variable airflow obstruction with features of atopic asthma, chronic bronchitis and emphysema [19]. Ghebre et al. showed that factor and cluster analyses of the sputum cytokine profiles in patients with COAD revealed three biological clusters that are separated by the expression of Th-2 cytokines [20]. There is also evidence that an allergic phenotype is associated with increased respiratory symptoms and risk of COPD exacerbations [21]. From a clinical perspective, identifying this group of patients is relevant because it has been reported that patients with ACOS have more frequent exacerbations, are more likely to have a severe exacerbation requiring hospitalisation, use more respiratory medications, and have more respiratory symptoms [22, 23]. However, there is endless discussion on how ACOS should be defined, and other authors have found that the ACOS phenotype was not clinically different at baseline, other than in the specific criteria used to define it [10], as we have observed here.
We have shown that a classification of COAD according to the presence of Th-2 inflammatory markers appropriately differentiates two groups of patients with different clinical expressions that can be considered treatable traits to guide therapy, irrespective of whether they had diagnoses of COPD or asthma. This suggests that it is reasonable to abandon the current approach of treating patients according to their diagnostic category, and to find treatable traits that justify effective interventions. Given the move towards personalised medicine [24], we propose here that a marker of Th-2 inflammation should be used to differentiate a pooled population of patients that share chronic airflow obstruction, making a new category of “overlapped” patients irrelevant. Using Th-2 inflammation in patients with COAD to determine therapy has some clear clinical implications: 1) it would identify patients who should receive ICS on top of long-acting single or dual bronchodilator therapy, reducing the excessive use of ICS in patients with COPD and thus reducing the side effects related to these drugs, e.g. pneumonia, osteoporosis, cataracts (it is worth noting that the NSA group showed a higher prevalence of osteoporosis, probably due to the long-term exposure to corticosteroids); 2) it would help to identify patients more likely to respond to biologic therapy; 3) it would provide a new perspective on non-eosinophilic asthma with chronic airflow limitation; and 4) it would end the continued discussion on the origin of airway diseases (Dutch and British hypothesis).
This Th-2 classification of COAD relies mainly on the use of blood eosinophil count, which is being widely employed in different trials with biological therapy aimed to block the Th-2 cascade. Thus, our inclusion criterion of 200 cells·µL−1 has been used to test the efficacy of benralizumab in eosinophilic COPD [25]. In keeping with this, Negewo et al. found that patients are unlikely to have sputum eosinophilia if their blood eosinophil count is <200 cells·µL−1 [12]. Moreover, Schleich et al. found a cut-off of 162 cells·µL−1 identified a sputum eosinophil count ≥3% in a COPD population of 155 patients, being 215 cells·µL−1 in those treated with high-dose ICS [26]. In view of these findings, the selected cut-off point to identify COPD-e (≥200 cells·µL−1) can be considered reasonable, although we are aware that a higher cut-off point would have a higher positive predictive value. By contrast, Wagener et al. [27] found that, in asthmatic patients, blood eosinophil counts had the highest accuracy in predicting sputum eosinophilia, with the best cut-off point of ≥270 cells·µL−1; this is why we decided to classify COAD as Th-2-high when the eosinophil count is ≥300 cells·µL−1.
Our work has several limitations that deserve comment. First, we used arbitrary cut-off points of blood eosinophil counts to recruit patients and to define their Th-2 profile, but we used the available published information that supports this view, as explained above. However, we were more stringent in the definition of Th-2-high, using a cut-off of 300 cells·µL−1, which is widely accepted [7]. Also, a large number of patients were receiving ICS and some of them were being treated with oral corticosteroids or omalizumab, which could have masked differences between groups and modified the expression of Th-2 markers. In addition, it is well known that active smoking can decrease FeNO in adults. Finally, the limit of 20 pack-years of smoking exposure in asthmatics could be misleading. However, by using this limit, we ensured that this phenotype overlapped the characteristics of smoking-related inflammation with those of baseline asthmatic inflammation.
Conclusions
We have shown that ACOS is an entity that might have different faces with different therapeutic approaches. We propose an easy-to-apply method to look at COAD using blood eosinophil counts that can separate two groups of patients with different clinical characteristics who require different therapeutic approaches. This proposal needs to be validated in further studies, including clinical trials, to demonstrate the usefulness of this approach.
Supplementary material
Supplementary Material
Please note: supplementary material is not edited by the Editorial Office, and is uploaded as it has been supplied by the author.
Supplementary material ERJ-02397-2016_Supplement
Disclosures
Supplementary Material
B.G. Cos#237;o ERJ-02397-2016_Cosio
M. Miravitlles ERJ-02397-2016_Miravitlles
J.J. Soler-Catalunya ERJ-02397-2016_Soler_Catalunya
Acknowledgements
The authors are grateful to all the patients who participated in the study. A number of investigators that contributed to the study logistics are listed in the supplemental material.
Authors’ contributions: B.G. Cosío and L. Pérez de Llano designed the study, recruited patients, analysed the results and wrote the manuscript. A. Lopez Viña, A. Torrego, J.L. Lopez-Campos, J.B. Soriano, E. Martinez Moragon, J.L. Izquierdo, I. Bobolea, J. Callejas, V. Plaza, M. Miravitlles and J.J. Soler-Catalunya recruited patients and reviewed the manuscript. The rest of the CHACOS study team recruited patients.
Footnotes
This article has supplementary material available from erj.ersjournals.com
Support statement: The project was endorsed by the COPD and Asthma Research Board of the Spanish Society of Respiratory Medicine (SEPAR). The project was partially funded by the Fondo de Investigaciones Sanitarias, Instituto de Salud Carlos III, Ministerio de Economia y Competitividad (FIS 15/01263) and by an unrestricted grant from Chiesi Pharmaceutici SpA. Chiesi had no role in the study design, data collection, data analysis, data interpretation, writing of the report, or in the decision to submit the article for publication. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication. Funding information for this article has been deposited with the Crossref Funder Registry.
Conflict of interest: Disclosures can be found alongside this article at erj.ersjournals.com
- Received December 6, 2016.
- Accepted March 2, 2017.
- Copyright ©ERS 2017
References










