





Abstract
Extended antithrombotic prophylaxis beyond hospitalisation may be beneficial in elderly, medically ill patients http://ow.ly/udyj304QvNo
To the Editor:
Compelling evidence suggests that the risk of pulmonary embolism and deep-vein thrombosis (DVT) persists after hospital discharge in acutely ill medical patients [1]. However, results of available studies did not support the routine use of extended-duration thromboprophylaxis in this setting [2–5].
Due to their higher baseline risk of venous thromboembolic events (VTE), older patients (≥75 years) may benefit more from an extended period of antithrombotic prophylaxis. However, this potential benefit may be offset by a higher risk of bleeding complications associated with the use of antithrombotic prophylaxis in this population.
To clarify this issue, we performed a pooled analysis of randomised controlled trials (RCTs) that assessed the efficacy and safety of the extended-duration thromboprophylaxis in different age classes (<75 years and ≥75 year).
RCTs evaluating the safety and efficacy of extended-duration thromboprophylaxis (EDT) versus standard thromboprophylaxis in acutely ill medical patients were searched in major databases (up to July 2016). Studies were considered and included only if separate data on patients with <75 years of age and those with an age ≥75 years were reported. The efficacy outcome was VTE and VTE-related death prevention; the safety outcome was represented by the occurrence of major bleeding. Pooled odds ratio and 95% confidence intervals were calculated for each outcome using a random effects model. The pooled number needed to treat (NNT) and the number needed to harm (NNH) were calculated for significant differences.
Three [2, 4, 5] of the four RCTs evaluating the safety and efficacy of EDT in acutely ill medical patients provided separate data according to different age groups. Of these, one study evaluated enoxaparin [2] as experimental drug, one rivaroxaban [3] and one betrixaban [5] for a total of 21 577 patients. Among enrolled patients, 10 008 (46.4%) had an age ≥75 years. All the three RCTs [2, 4, 5] provided data on the efficacy outcome defined by the prevention of composite of symptomatic or asymptomatic proximal DVT (and symptomatic distal DVT in the Magellan [4] and Apex [5] studies), symptomatic pulmonary embolism and VTE-related death. In contrast, two studies [2, 5] reported major bleeding and one [4] reported major and clinically relevant non-major bleedings.
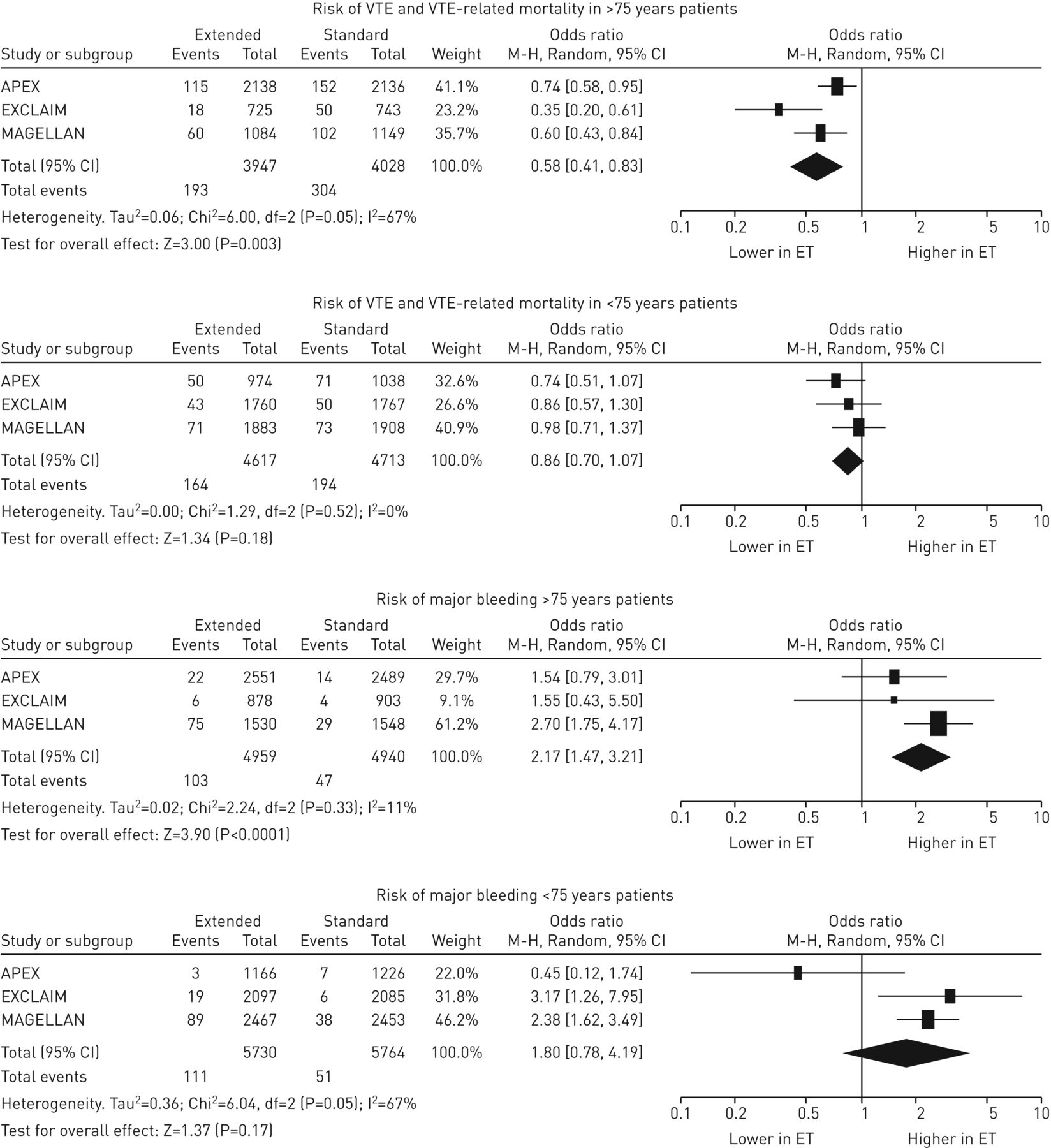
Among patients aged ≥75 years, the risk of VTE or VTE-related death was 4.5% (95% CI 3.1%–6.4%) during EDT and 7.6% (95% CI 6.4%–8.9%) during standard thromboprophylaxis with a corresponding odds ratio of 0.58 (95% CI 0.41–0.83), and a NNT to prevent an episode of VTE or VTE-related death of 38 (figure 1). The risk of bleeding was 1.5% (95% CI 0.4%–5.9%) in EDT patients and 0.8% (95% CI 0.3%–2.2%) in standard thromboprophylaxis patients with a corresponding odds ratio of 2.17 (95% CI 1.47–3.21), and resulting in a NNH of 350 for major bleeding when we considered only the two studies that provided separate data for this outcome (figure 1).

{kind=link}
Summary of efficacy and safety endpoints according to different age groups. VTE: venous thromboembolic events; M–H: Mantel–Haenszel; random: random-effects model; ET: extended thromboprophylaxis; APEX: Acute Medically Ill Venous Thromboembolism Prevention with Extended Duration Betrixaban; EXCLAIM: Extended, Clinical Prophylaxis in Acutely Ill Medical Patients; MAGELLAN: Multicenter, Randomized, Parallel Group Efficacy and Safety Study for the Prevention of VTE in Hospitalized Acutely Ill Medical Patients Comparing Rivaroxaban with Enoxaparin.
In those aged <75 years, the risk of VTE or VTE-related death was 3.6% (95% CI 2.4%–5.4%) in EDT patients and 4.2% (95% CI 2.5%–6.9%) in standard thromboprophylaxis patients (OR 0.86, 95% CI 0.70–1.07) (figure 1). Bleeding episodes were reported in 1.0% (95% CI 0.3%–3.9%) of EDT patients and in 0.7% (95% CI 0.2%–1.9%) of standard thromboprophylaxis patients (OR 1.80, 95% CI 0.78–4.19) (figure 1).
Results of our pooled analysis suggest a different trade-off of extended antithrombotic prophylaxis according to age. In particular in patients aged ≥75 years, extended prophylaxis appeared associated with a significantly reduced incidence of the composite efficacy endpoint of VTE or VTE-related death only partially offset by a significant increased risk of major bleeding complications. Indeed, only 38 patients aged ≥75 years have to be treated to prevent one episode of VTE or VTE-related death whereas about 350 patients have to be treated to cause one additional major bleeding event suggesting a potential benefit of an extended period of antithrombotic prophylaxis in this subgroup of patients. On the other hand, in younger patients extended prophylaxis did not result significantly associated either with a reduced risk of VTE or VTE-related death or with an increased risk of major bleeding events not supporting its use in this subgroup of patients.
Our findings should be considered hypothesis-generating only, since we pooled the results of efficacy and safety of extended prophylaxis in different age groups and patients were not randomised accordingly. Thus, differences in baseline characteristics of these patients could not be excluded. Furthermore, our conclusions were based on the results of only three studies and clinical weight of the efficacy endpoint (that included also asymptomatic events) may be lower compared to that of safety endpoint (major bleeding events). Finally, different compounds, with some differences in terms of mechanisms of action, have been tested for EDT and differences in efficacy and safety of these compounds in this setting could not be excluded. Thus, extreme caution is necessary in data interpretation.
In conclusion, results of our pooled analysis suggest a potential benefit of extended antithrombotic prophylaxis in elderly medical ill patients. However, other properly designed RCT are warranted to confirm our preliminary findings.
Footnotes
Conflict of interest: None declared.
- Received September 25, 2016.
- Accepted October 2, 2016.
- Copyright ©ERS 2017










